
A NEW PARADIGM IN MEDICINE
Scientific bases
Fundamentals of Methodology
Pre-clinical and clinical research
Per minima ad maxima
Physiological Regulating Medicine (PRM) was born from the merging of Molecular Biology with Psycho-Neuro-Endocrine-Immunology (PNEI), and was developed in recognition of research results in the field of the pharmacology of low doses.
Physiological Regulating Medicine is a person-centered Medicine, based on three guiding principles:
- to treat the man and not just the disease;
- to act on the causes and not just the symptoms;
- to consider man as a whole mind-body and in his individuality.
Physiological Regulating Medicine starts from an original idea in the medical field: to bring back a sick organism to the original physiological condition through the use of the same biological molecules normally present in the body and that, in healthy conditions, monitor and guide body functions.
In fact, many of these molecules are known and studied by Molecular Biology, which defines them as signaling (messenger) molecules, substances that are able to transport to different cells in the body the “correct instructions” for their best operation.
These molecules are neuropeptides, hormones, and cytokines, along with growth factors, fundamental regulatory molecules, and tissue stimulating molecules.
Signaling Molecules and the P.N.E.I. network
Since the 1970s, research in the fields of Physiology and Molecular Biology has given increasing evidence to the critical role of signaling molecules in all physiological and pathological processes.
It is recognized that these substances play a decisive role in determining the state of health or of illness and it is now established that each disease is the expression of mutated concentrations, in excess or deficiency, of these substances; all the medical research is moving toward the study of signaling molecules, which determine the fate in a positive (healing) or negative (progression) way of numerous pathological conditions, and the possibility of their application for therapeutic purposes.
In hand with the acquisitions on the signaling molecules, in the last years we have witnessed in the medical field, the gradual abandonment of the separatist and scotomized conception of the biological functions of the body, giving way to a more unified one in accordance with the guiding principles of Psycho-Neuro-Endocrine-Immunology (P.N.E.I.) [1-4].
P.N.E.I. approach represents a genuine paradigm shift in Medicine: from a strictly biomedical and specialized view of health and disease to a deeply interdisciplinary one. The main unifying P.N.E.I. element is identified in the cross-talk between the psycho-neuroendocrine Systems and the immune System (Figure 1).
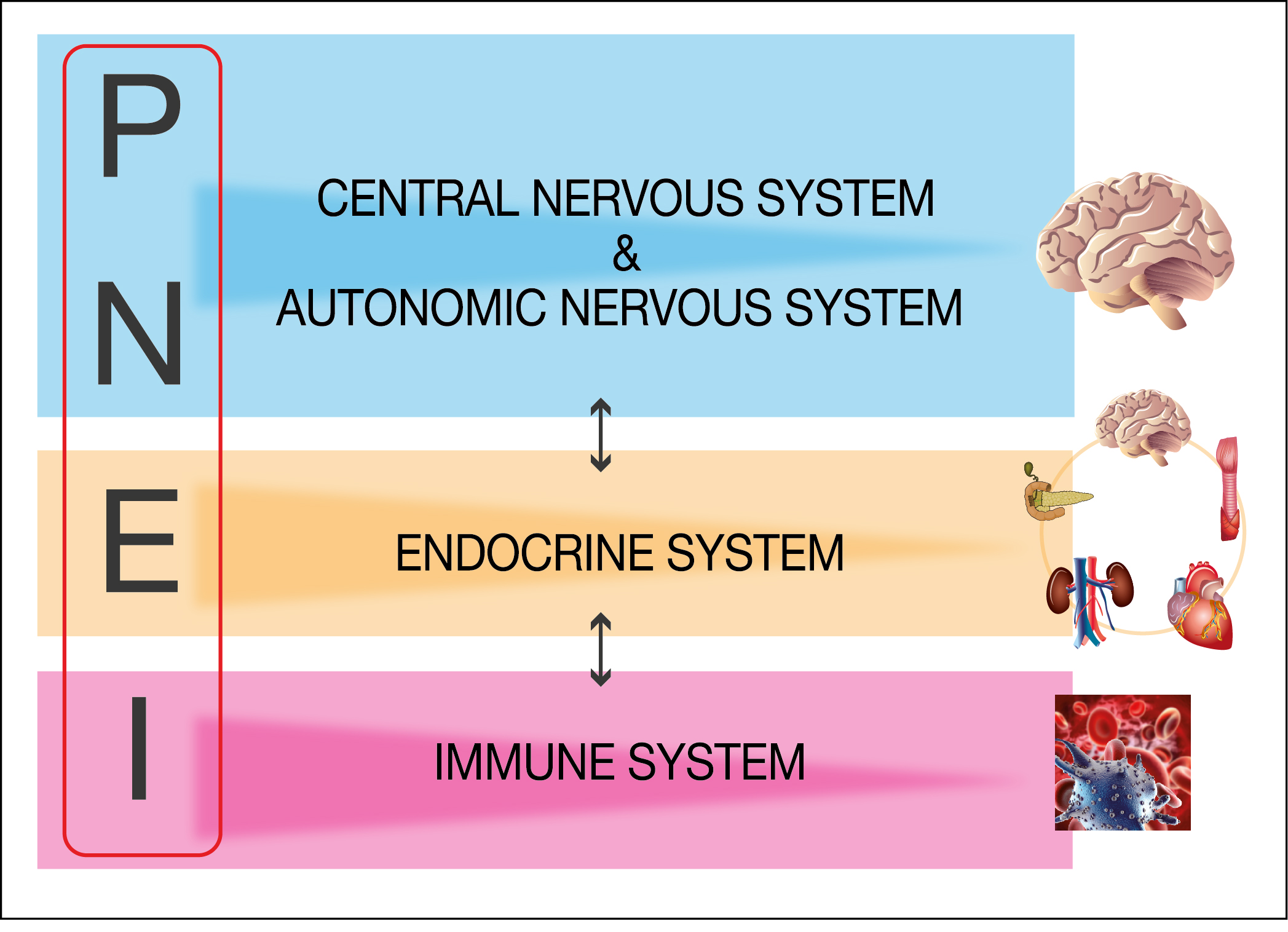
This sophisticated cross-talk is mediated by a complex network of signaling molecules (cytokines, hormones, neuropeptides and growth factors) which are the vehicle of the biological information necessary for the complex and efficient regulation of cellular responses to stimuli. An altered cross-talk due to an imbalance between specific signal molecules is fundamental, for example, in inflammatory, allergic and autoimmune diseases onset [5-7]; restoring the physiological concentration of signaling molecules is the key point to recover the homeostatic equilibrium.
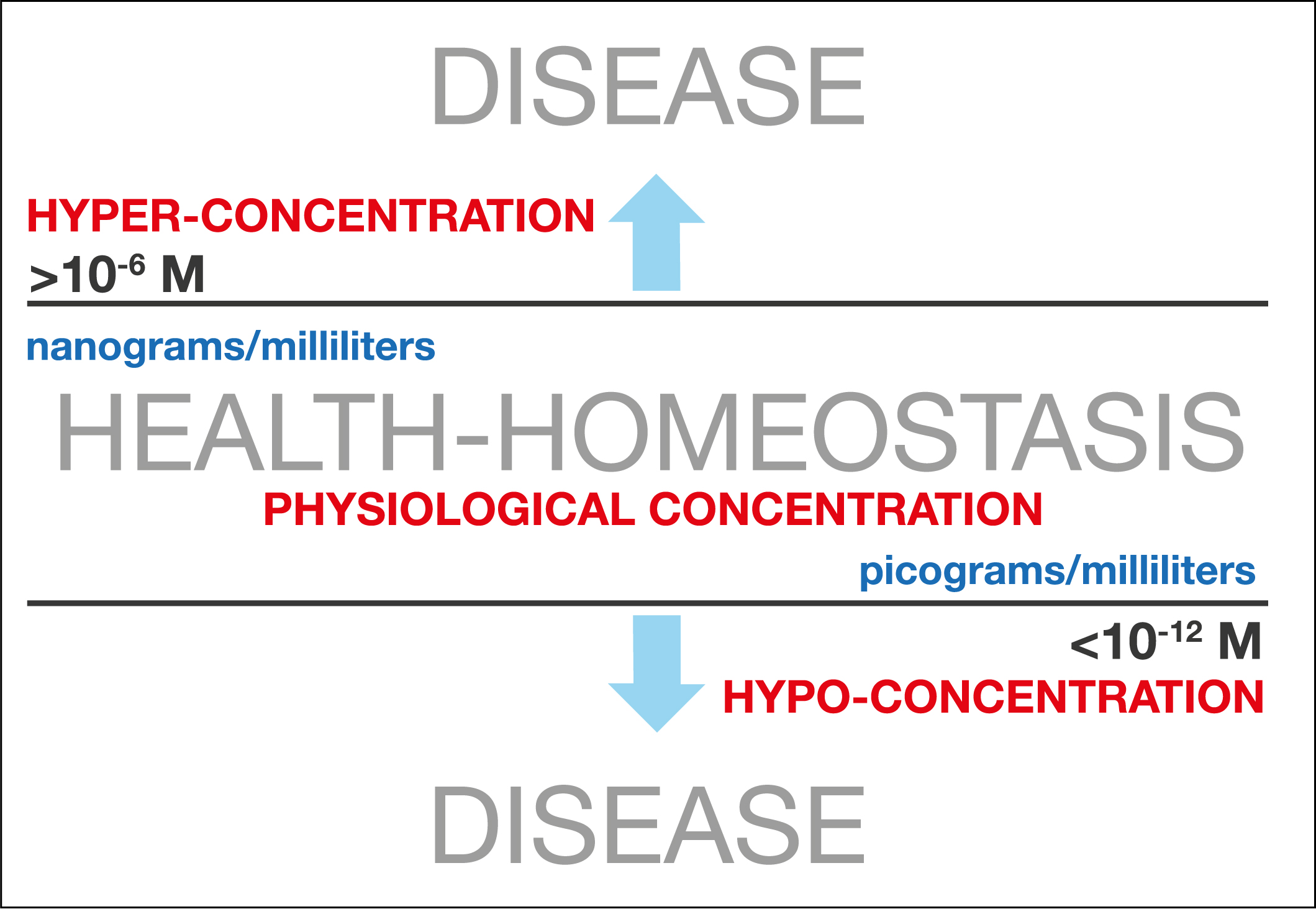
In homeostatic conditions (corresponding to a healthy state), the concentrations of these molecules in the Extra-Cellular Matrix (ECM) [8-9]are comprised in a specific physiological range (from nanograms/ml to picograms/ml) and diseases can be considered as expressions and consequences of changed concentrations of these fundamental substances [10-13] (Figure 2).
The use of biological molecules, which control and drive cellular functions in order to restore the original homeostatic physiological condition, is the core of Physiological Regulating Medicine.
For a deep understanding of Physiological Regulating Medicine, it is necessary to consider some key points related to cross-talk between the systems of P.N.E.I. network (and between the cells) mediated by signaling molecules:
- The cross-talk between cells, organs and systems is always bi-directional, such as the effects of the alteration of the cross-talk itself [14-16];
- The intercellular signaling occurs through the diffusion of signaling molecules in the ECM: states of pathological alteration of the ECM lead to the deterioration in the quality of the communication between cells and, in general, between organs and Systems [17, 18];
- The ligands-receptors interaction is crucial for the efficacy of the signal transduction in terms of quality and potency: substrate concentration and binding properties such as affinity and saturation phenomena are key parameters [19, 20].
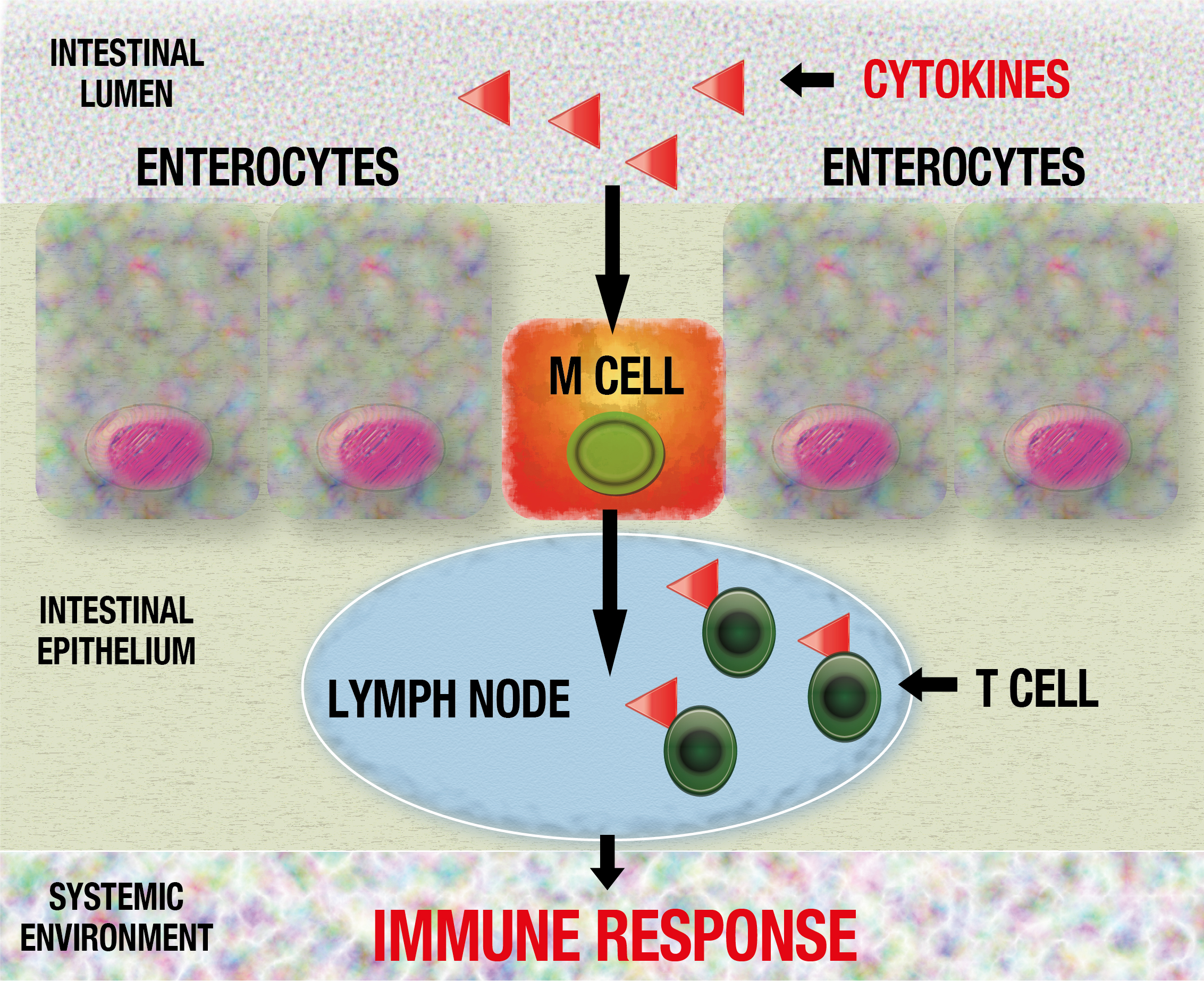
The signaling molecules used in PRM are orally administered and their activity is systemic (acting on complex cell signaling pathways). Scientific literature reports that cytokine oral intake is effective in modulating immune response [21-23]; a possible action mechanism involves M cells at intestinal epithelium level. Signaling molecules are taken by M cells from intestinal lumen and presented to immune T cells within Peyer’s patches lymph nodes [24] inducing an appropriate immune response (Figure 3).
How “low” must a low dose be (to be effective and safe)?
A critical point of signaling molecules (and peptides in general) oral administration is represented by their low bioavailability (typically less than 1-2%); an effective drug delivery system is requested in order to improve this key parameter. The use of physiological low doses (nanograms-picograms) (Figure 2) per os in PRM is made possible by the application of SKA technology (Sequential Kinetic Activation), a particularly sophisticated drug delivery system, based upon the principle of release activity, that is the ability of the basic substance to release its activity in the aqueous milieu) [25], which allows the sub-nanomolar concentration to be active, even below the actually considered minimum effective dose, with therapeutic results comparable to those induced by high concentrations.
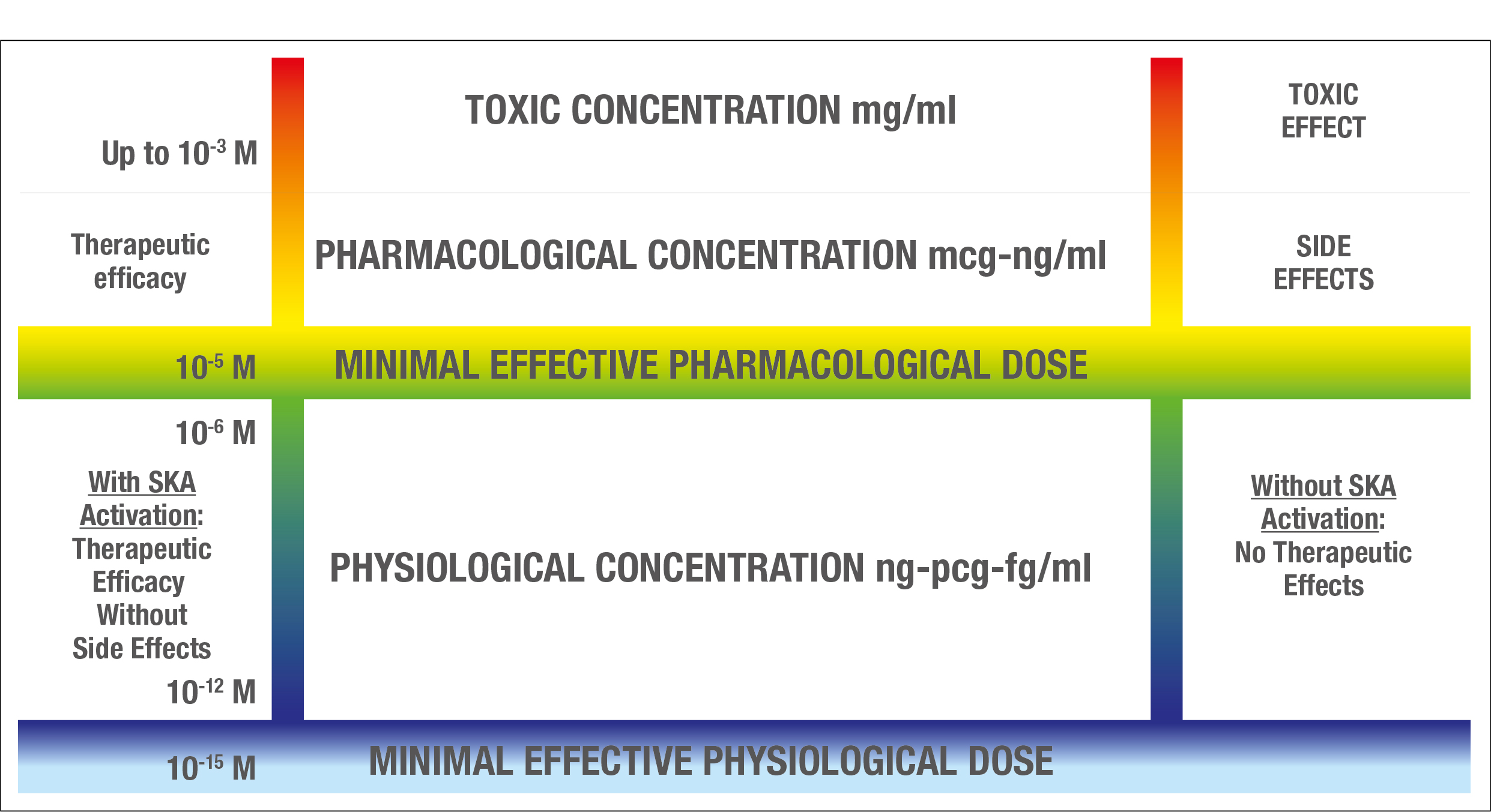
The action mechanism of SKA low dose cytokines, hormones, neuropeptides and growth factors consists in sensitization or activation of some units of cellular (or plasmatic) receptors in virtue of their high dilution, in their physiological working range between 10-6 molar (microgram) for hormones [8] and 10-12 molar (picogram) for the other signaling molecules [9] (Figure 4). Low doses of signaling molecules can trigger their specific receptors modulating intracellular control pathways driven by key molecules, such as SOCS-1 (26). These receptors sensitizations and activations allows the trigger of chain reactions (complex systems) and a restart of the biological function of the whole P.N.E.I. network.
SKA low dose molecules work by bringing to the system information able to activate auto-regulation mechanisms.
Given these premises, from the clinical point of view, the therapeutic approaches are:
- To restore the homeostasis of a pathologically down-regulated cellular pathway administering the same cytokine, hormone, neuropeptides or growth factor (low dose SKA) that is physiologically involved in the cellular signaling;
- To use antagonistic molecules (low dose SKA) in order to down-regulate the molecules pathologically up-regulated, restoring their homeostatic concentration via negative feedback mechanisms, according to the principle of “opposing” molecules.
The ability to correct, for example, alterations of the immune System with the use of cytokines or endocrine disorders with the use of hormones, represents one of the most fascinating and innovative research fields in Molecular Biology applied to Medicine; unfortunately the clinical application of this knowledge has always been brought to a standstill by the side effects that these substances show when used at high doses, those normally used until now.
Bio-Tech and low dose
The latest knowledge in the field of biotechnology production of human recombinant proteins allowed researchers to realize medicines of highest quality and efficacy. The PRM low dose medications are biotech natural pharmaceuticals based on sub-nanomolar concentrations of human recombinant proteins. It is crucial in this new generation of medicines the precise range of low doses used. They are corresponding to the physiological concentrations of signaling molecules. Thanks to the aforementioned pharmaceutical technique SKA, it is now possible to use sub-nanomolar concentrations of hormones, neuropeptides, cytokines and growth factors with therapeutic results comparable to those induced by high concentrations of them but without side effects.
The SKA method inaugurates a new era within the possibility of clinical use of signaling molecules; the “scientific dream” to use biological molecules such as cytokines, hormones, neuropeptides or growth factors at low dosages (the only possible not to induce side effects) becomes today possible thanks to the particular pharmaceutical procedure used in the production of these molecules. A new frontier in the fields of pharmaceutical industry and Molecular Biology is born and it is developing all over the world; Italian researchers and Italian industry are cutting-edge in this field.
References
- Ader R, Cohen N, Felten DL (1987) Brain, behavior, and immunity. Brain Behav Immun 1(1): 1-6.
- Ader R, Felten D, Cohen N (1990) Interactions between the brain and the immune system. Annu Rev Pharmacol Toxicol 30: 561-602.
- Ader R, Cohen N (1993) Psychoneuroimmunology: conditioning and stress. Annu Rev Psychol 44: 53-85.
- Ader R, Cohen N, Felten D (1995) Psychoneuroimmunology: interactions between the nervous system and the immune system. Lancet 345(8942): 99-103.
- Haroon E, Raison CL, Miller AH (2012) Psychoneuroimmunology meets neuropsychopharmacology: translational implications of the impact of inflammationon behavior. Neuropsychopharmacology 37(1): 137-62.
- Ngoc PL, Gold DR, Tzianabos AO, Weiss ST, Celedón JC (2005) Cytokines, allergy, and asthma. Curr Opin Allergy Clin Immunol 5(2): 161-6.
- Lourenço EV, La Cava A (2009) Cytokines in systemic lupus erythematosus. Curr Mol Med 9(3): 242-54.
- Vandenberg LN, Colborn T, Hayes TB, Heindel JJ, Jacobs DR Jr, et al. (2012) Hormones and endocrine-disrupting chemicals: low-dose effects and nonmonotonic dose responses. Endocr Rev 33(3): 378-455.
- Biancotto A, Wank A, Perl S, Cook W, Olnes MJ, et al. (2013) Baselinelevels and temporal stability of 27 multiplexed serum cytokine concentrations in healthy subjects. PLoS One 8(12):e76091.
- Reeves R, Leonard WJ, Nissen MS (2000) Binding of HMG-I(Y) imparts architectural specificity to a positioned nucleosome on the promoter of the human interleukin-2 receptor alpha gene. Mol Cell Biol 20(13): 4666-79.
- IshiharaK, Hirano T (2002) Molecular basisof the cellspecificity of cytokineaction. Biochim Biophys Acta 1592(3): 281-96.
- Commins SP, Borish L, Steinke JW (2010) Immunologic messenger molecules: cytokines, interferons, and chemokines. J Allergy Clin Immunol 125(2 suppl 2): S53-72.
- Bacchus W, Aubel D, Fussenegger M (2013) Biomedically relevant circuit-design strategies in mammalian synthetic biology. Mol Syst Biol 9: 691.
- Weigent DA, Blalock JE (1995) Associations between the neuroendocrine and immune systems. Journal of Leukocyte Biology 58(2): 137-150.
- HaddadJJ (2008) On the mechanisms and putative pathways involving neuroimmune interactions. Biochem Biophys Res Commun 370(4): 531-5.
- De la Fuente M (2014) Editorial: crosstalk between the nervous and the immune systems in health and sickness. Curr Pharm Des 20(29): 4605-7.
- Morrell NW, Adnot S, Archer SL, Dupuis J, Jones PL, et al. (2009) Cellular and molecular basis of pulmonary arterial hypertension. J Am Coll Cardiol 54(1 Suppl): S20-31.
- Bollyky PL, Bogdani M, Bollyky JB, Hull RL, Wight TN (2012) The role of hyaluronanand the extracellular matrix in islet inflammation and immune regulation. Curr Diab Rep 12(5): 471-80.
- Borroni EM, Mantovani A, Locati M, Bonecchi R (2010) Chemokine receptors intracellular trafficking. Pharmacol Ther 127(1): 1-8.
- Farrell MS, Roth BL (2013) Pharmacosynthetics: Reimagining the pharmacogenetic approach. Brain Res 1511: 6-20.
- Burnett AF, Biju PG, Lui H, Hauer-Jensen M (2013) Oral interleukin 11 as a countermeasure to lethal total-body irradiation in a murine model. Radiat Res 180(6): 595-602.
- Hanson ML, Hixon JA, Li W, Felber BK, Anver MR, et al. (2014) delivery of IL-27 recombinant bacteria attenuates immune colitis in mice. Gastroenterology 146(1): 210-221.
- Forster K, Goethel A, Chan CW, Zanello G, Streutker C, et al. (2012) An oral CD3-specific antibody suppresses T-cell-induced colitis and alters cytokine responses to T-cell activation in mice. Gastroenterology 143(5): 1298-307.
- Yun Y, Cho YW, Park K (2013) Nanoparticles for oral delivery: targeted nanoparticles with peptidic ligands for oral protein delivery. Adv Drug Deliv Rev 65(6): 822-32.
- O. I. Epstein. Release-Activity: A Long Way from Phenomenon to New Drugs. Bulletin of Experimental Biology and Medicine November 2012, Volume 154, Issue 1, pp 54-58
- Castiglioni S, Miranda V, Cazzaniga A, Campanella M, Nichelatti M, Andena M, Maier JAM. Femtograms of Interferon-γ suffice to Modulate the behavior of Jurkat cells: A new light in immunomodulation. Int. J. Mol. Sci. 2017;18:2715
